Trigger Warning: Medically Fragile Infants & Congenital Heart Disease (CHD)
This case study explores the experiences of medically fragile infants with congenital heart disease (CHD), including complex medical interventions, prolonged hospitalizations, and the challenges faced by families and caregivers. It discusses life-threatening conditions, intensive medical procedures, and the emotional and ethical complexities of neonatal and pediatric care.
I recognize that this content may be distressing, particularly for those with personal or professional connections to medically complex infants. Please prioritize your well-being—feel free to step away if needed and engage with the material in a way that feels safe for you.


Providing a sense of progression and empowering parents in their baby's care.
Challenge:
How might we ease transitions and provide a sense of progress for pediatric caregivers in a complex medical journey?
This project aimed to improve the pediatric congenital heart disease discharge process for medically fragile babies and their families, by transitions and providing a sense of progress in a stressful and unpredictable medical journey.
Timeline:
January 2021- June 2021
Client:
Role:
TX Center for Ped CHD at Dell Med
Lead Service Designer/Researcher
Outcome:
A coordinated system of tools and processes were designed to enhance communication and align efforts across patient families and care team members.
Our team designed a coordinating workbook and care board toolset to enhance communication and goal tracking, while also reinforcing process alignment and collaboration across patient family and care team members to improve experience.
A four month clinical pilot was conducted and data results showed:
-
64% of parents agreed or strongly agreed that prototypes helped track their child’s progress and
-
90% would recommend to others.
-
This work has also increased the likelihood of survival in babies with CHD BY 40% outside of medical confines.
-
Our design team also co-authored a peer- reviewed abstract with the clinical team sharing our work. It was published by the American Academy of Pediatrics in January 2022.
-
Implementation of the parent workbook has been launched at the Heart Center in English and Spanish, wide scale production is currently underway.
Impact:
Prototypes provide overarching structure and progressive guideposts that engages users where they are, and helps everyone feel ready to transition home.
The Texas Center for Pediatric and Congenital Heart Disease is the only pediatric program in Central Texas offering comprehensive heart care for newborns, infants, children, and adolescents. While the program has many distinguishing features, the discharge process for single ventricle (SV) babies, a critical subtype of congenital heart disease (CHD), has remained challenging with such a wide range of patient, family, and care team needs to account for.
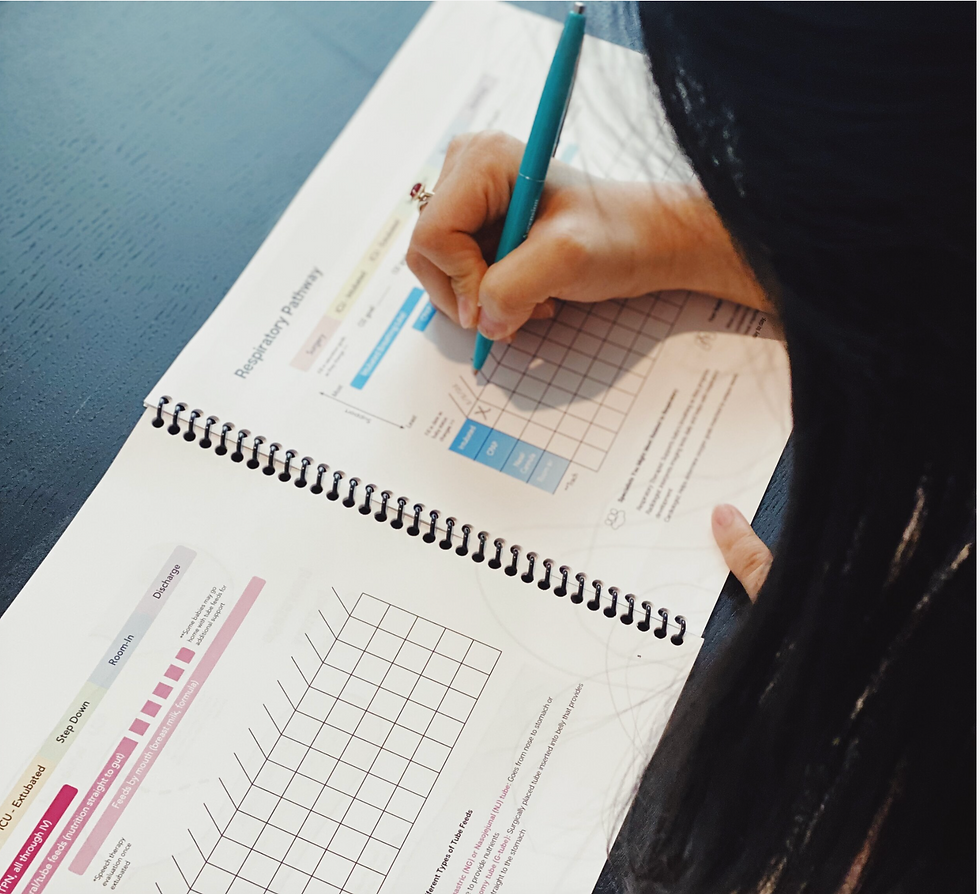
We saw an opportunity to provide more structure and communication earlier in the process, thinking about discharge as more than just a discrete event, but rather a series of steps throughout the 3 weeks to 6 months hospitalized after surgery. Our workbook and care board function as a coordinated system, introducing both overarching structure and progressive guideposts into the clinical setting that all users can follow, that reinforce a sense of progress so everyone feels ready to transition home.

Designing a Coordinated System
New concept illustration showing how the toolset works together.

Clinical Care board Prototype
Caregiver Workbook Excerpt
8.5 Inch, spiral bound, full color printing
2X3 ft, Full size mock-up treated with whiteboard laminate material to simulate real world use.

Design Blueprint
High level blueprinting outlining the actions and tools needed to guide pilot planning



Introduction:
1 in every 100 babies born in the United States will be diagnosed with congenital heart disease (CHD), and a quarter of those will require surgery or other procedures in their first year of life. Patients that are diagnosed with single ventricle CHD are especially vulnerable and face years of complex medical care. Although outcomes have improved significantly over the last decade, mortality remains a serious concern.
The first surgery occurs right after birth and is followed by inpatient hospitalization lasting from 3 weeks to 6 months in the intensive care unit. During this period babies are medically fragile and this takes a toll on both patient families and care team members. Patients receive care from a very large team of care team upwards of 60 people each hospital stay. With so many care providers involved—and thus multiple priorities in play— discharge quickly become complicated.

Research Process:

At the start of our research we wanted to understand how the discharge process worked, how it felt to patient families and care team members, and what opportunities and challenges existed to direct our efforts.
Key Research Questions:
-
How does the discharge process work now?
-
What/ How does the process feel like?
-
What works well and what opportunities for improvement exist
Data Synthesis Methods:
-
Journey Mapping
-
Artifact Analysis
-
Affinity Diagramming


Understanding the journey
The diagnosis of single- ventricle (SV-CHD) starts years of complex medical interventions. These infants are medically fragile and require multiple surgeries and hospitalizations in the Cardiac intensive care unit. (CVICU)
Interstage Journey Map:
Journey map shows the interstage period, occurring between first surgery performed just after birth and second surgery approximately 6 months later. This is a low fidelity visualization I created during the research phase to help the design team better understand the dense clinical information we had gathered.

-
Journey mapping and artifacts analysis were paramount in helping us to navigate and hone in on our insights and prototypes.
-
The journey map empowered us to fully grasp each stage of the process, understanding how actions and milestones are interconnected. By identifying touch points, pain points, gain points, and gaps in care, we gained invaluable insights to refine our approach, close gaps in care and enhance the overall experience.

-
The gingerbread man is placed in all patient rooms to help caregivers understand and visualize placement of medical devices and tubing.
-
The care team made it clear to the families and us that if they do not pass this “Test,” they will not be discharged home.
-
However, written in blue ink on the bottom of the paper it states, “This is a learning experience, not a test.”
-
This message is highly confusing to caregivers.

"There was nowhere to look and see what we had accomplished or how far we still had to go."
- Single Ventricle Heart Patient
Insights Developed:
At the start of our research we wanted to understand how the discharge process worked, how it felt to patient families and care team members, and what opportunities and challenges existed to direct our efforts. Several core insights emerged:

Every parent is responsible for learning and responding to red flag warning signs of distress. This sign is posted on every single ventricle baby's door contributing to a heightened sense of alert.
The high stakes of caring for a medically fragile child complicates roles and responsibilities
Having a single ventricle baby means that parents are on point for learning complex clinical information. Instead of focusing on the basics of routine baby care, parent attention is on how to be healthcare providers for the home environment. This complicates the typical doctor-patient relationship where the doctor is viewed as the expert, and it muddies the parent role, where the parent always knows best.
Every child's journey is unique, but families still need guideposts along the way.
There is no single CHD journey and whatever that path might be, it is often not linear. Families expressed a desire to have a better idea of what they might face and ability to track goals they were working toward. From the care team, we learned that the path is often unpredictable but there were also key milestones that anchor the journey.

A Single ventricle baby is hooked up to medical equipment early in the hospital stay
(photo credit: Jose Coclucci)

Caregiver handout detailing room-in, the period just before discharge where care skills are demonstrated. “This is a learning experience not a test," hand written hints at potential team misalignment.
Being in the ICU means it's never not an emergency, even as clinical status changes.
When babies progressed through their first hospital stay in the past, step down in acuity was marked by changing physical location to different floors. But due to changes in safety protocols single ventricle patients now stay in the ICU the entire interstage period. This makes it difficult to transition clinically and psychologically for parents and care team members, leaving everyone on high alert even as patients become more medically stable over time.
Both caregivers and care team yearn for consistency and standardization to alleviate anxiety.
There is a lot that is outside of a parent’s control. Inconsistent messaging and frequent schedule changes amplify anxiety that might already be felt. In our research we found that standardization and efficient team communication are key to improve care coordination. There are workarounds everywhere in the environment, illustrating how the care team is seeking more structure.

Several care team workarounds exist to help streamline and organize discharge, including this handwritten prep list detailing steps taken and who is on point.

Several care team workarounds exist to help streamline and organize discharge, including this handwritten prep list detailing steps taken and who is on point.
Disparities in resource and care delivery make everything more difficult.
Our last insight centers on how all of these challenges are exacerbated by barriers related to social determinants of health. For example, being in Central Texas, we heard over and over again how Spanish-speaking families don’t have the same experience as those who speak English. On multiple levels, parents are grappling with meeting complex demands with limited means and support.



"We spend a lot of time with these families and want to do everything we can to help them be successful."
-Pediatric Cardiologist
Ideation:
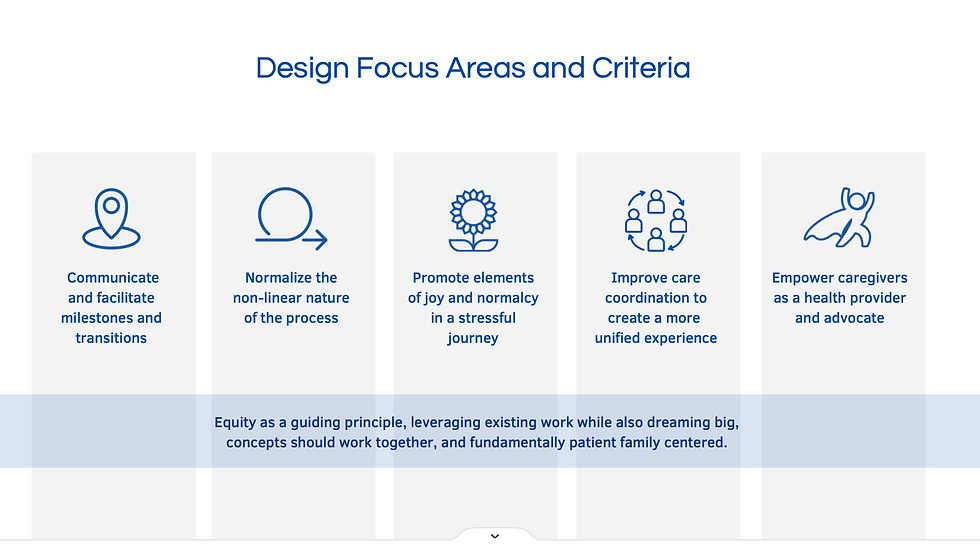
As a team we ideated in response to several design goals, articulated as “how might we” statements, and came up with many potential concepts which we narrowed down to an initial short list.
Using a 2x2 matrix activity we asked the client team to individually place each of the final design concepts and then compared the ranking followed by facilitated open discussion. This allowed us to come to shared vision and provided guidance regarding which concepts should be prioritized (depicted in yellow).

-
Better facilitate milestones and transition during interstage
-
Normalize the non-linearity nature of the process
-
Promote elements of joy and normalcy as new parents
-
Improve care coordination and create a more seamless experience
-
Empower caregivers in their new roles as care stewards
How might we.....

Our early thoughts:
Heart Family Storybooks and Keepsake Journal
A series of children’s storybooks offered to families either before birth or throughout the duration of their inpatient stay. Stories are based off real single ventricle patient experiences, written and illustrated in the style of a children’s book. Families will also be able to create their own version as a keepsake, chronicling their journey as they progress through the interstage period.
CaregiverWorksheet
This worksheet provides an overview of the journey during interstage. Key milestones, people, activities, and supplies are organized by clinical phase. Personal goals and unique factors can be documented to challenge a more linear timeline. Bonding tips tailored to baby status are also noted along with an emotion tracker to encourage open communication and self care. Interwoven quotes aim to validate the caregiver experience.


Clinical Care Board
Care board changes externalize transition through changing clinical status, even when families remain in the same room throughout their stay. Color coding delineates phases and organizes key goals. A magnet piece is moved up or down to help caregivers track movement and shift mindset. Personal details like baby preferences have also been built in to encourage engagement and support care experience.
Pivot Point
After speaking to the care team, their main request was a patient-oriented roadmap to enable caretakers to better understanding the journey is unique for every baby and it is a non-linear process.







"Parents are thrown a lot of information. The workbook helps welcome parents while preparing them for home from the start."
-ICU Bedside Nurse
Prototyping and Testing
-
To test our concepts we created low fidelity prototypes and engaged patient families and care team members for feedback. Facilitating talk aloud and co-creation sessions it helped us understand that although our initial designs addressed the challenge of information overload and lack of direction, more clinical detail was needed to make the biggest impact. We came to realize just how medically savvy heart parents are expected to be and that more than anything they needed tools to help them get there.
-
In response to the feedback we evolved the worksheet concept into a multipage workbook for families that were organized in a variety of ways including time, clinical phase, and organ system. We also changed the clinical care board so it organized actions based on frequent patient touch points and translated this into corresponding pages in the caregiver workbook. Both prototypes connect with a care team focused discharge checklist that helps the care team organize their clinical tasks behind the scenes
Testing Feedback
-
Worksheet and care board prioritized over storybooks by both patient families and care team - though met with positive emotional response
-
Needed to be more clinically detailed
-
Tools could more directly standardize clinical processes currently under development
-
Desire for the “DIY” storybook elements to be combined with clinical tracking tools
Designing a Coordinated System
New concept illustration showing how the toolset works together
8.5 Inch, spiral bound, full color printing
Caregiver Workbook Excerpt
Clinical Careboard Mock-up
Mock-up of care board placed where it would normally hang in the patients room.
Implementation:

Theory of Change:
Outline of short, mid, and long term outcomes through design implementation.
Service Outcome
In the end, we developed an interactive, highly detailed workbook tailored to assist families in navigating the non-linear progression of their journey, while also ensuring moments of normalcy are maintained. Additionally, we incorporated the redesigned care board to delineate the various stages of their interstage journey during their hospital stay.
The care board and workbook feature color-coded stages aligned with medical pathways, incorporating familiar symbols such as the classic gingerbread man. Additionally, the workbook includes space for children to creatively express their own stories.

We were invited to speak at the heart conference to discuss out new designs and publish our work. Dell Children's decided to move forward with the design as well and apply it to other patient populations.
It is used regularly with families to this day.
What happened next?

Soul-food /Takeaways
Participating in this project was an extraordinary experience. Seeing its profound effect within such a sensitive community deeply resonated with the meaningful work I strive to pursue. Moreover, I want to extend my sincere appreciation to the incredible group of women I had the honor of working alongside—a team distinguished by their exceptional talent and unwavering supportiveness.
-
Throughout the project we have learned that it's important to seek full perspective early on and work iteratively in the process.
-
We also learned how to give space and kindness with sensitive topics/ families.
-
Throughout the process, I constantly asked “Who is the customer? Who is the user?” I came to understand that our “user” is an organization. That added layers of complexity because of the increased number of stakeholders, each one having their own needs and agendas. This came out during our usability interviews and manifested itself in thinking about different touchpoints/information.